
 Edit by: Brittni
Edit by: Brittni Reviewed by:
Reviewed by:  Written by:
Written by: 
Drug use during pregnancy is a severe problem worldwide because it exposes not only the woman but also her developing baby to harmful substances. Tobacco and alcohol are the most commonly abused substances, followed by marijuana and cocaine. Using drugs while pregnant and addiction is a grave concern because it puts two lives at risk.
Table Of Contents:

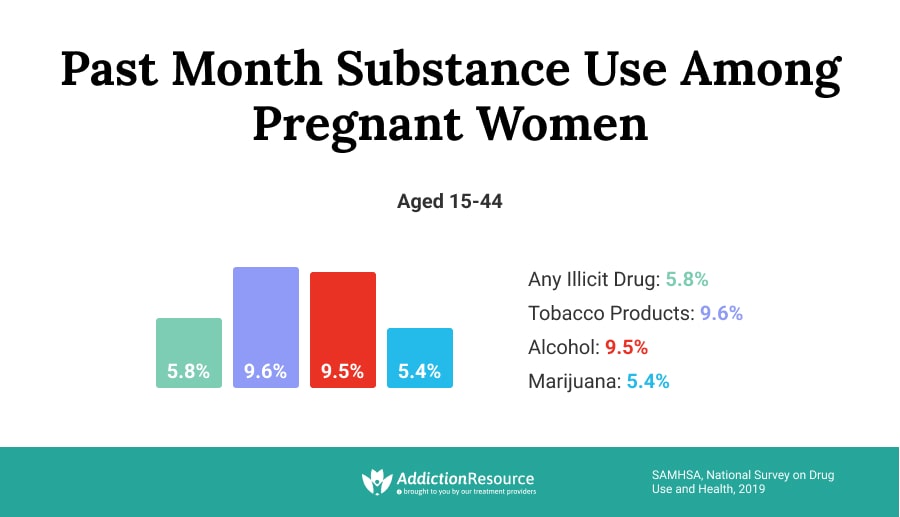
Substance use disorders are most prevalent in adolescents and young adults. It puts women of childbearing age (15 to 44 years old) at the greatest risk of developing an addiction. In fact, according to a nationwide survey on drug use in 2012, almost 16 percent of pregnant women smoked cigarettes, 8.5 percent drank alcoholic beverages, and nearly 6 percent used illicit drugs.
The effects of drugs and alcohol during pregnancy are terrifying, as it puts both a mother and a baby at serious risk. Therefore women should have all the information about the dangers to make the right decision for their safety and the safety of their future child.
Drug Use During Pregnancy Statistics
Effects of drugs and alcohol during pregnancy include many severe maternal and fetal health consequences. Nearly 90 percent of women on drugs are of reproductive age. SAMHSA provides some drug use during pregnancy statistics, stating that 5.4 percent of pregnant women between ages 15 and 44 are current users of illicit drugs. In pregnant teens (age 15 to 17), the rate of drug abuse is much higher at almost 15 percent. More than 8 percent of women report current alcohol use, and nearly 3 percent are binge drinkers. Tobacco use is also prevalent in pregnant women, and 1 in 14 pregnant women smokes cigarettes. It is evident that substance use disorders are rampant during pregnancy.
Let’s look at some facts and figures about addiction in pregnant women and drug use during pregnancy statistics in detail.
Tobacco Use
Data from the National Vital Statistics System in 2016 found that a little over 7 percent of women smoked cigarettes during their pregnancy. The study found that the prevalence of tobacco use is highest in the 20-24 years age group. American-Indians and Alaskan Natives have the highest incidence of tobacco abuse at almost 17 percent. Smoking during pregnancy is highest in West Virginia (more than 25 percent) and Kentucky (nearly 19 percent).
Smoking while pregnant is harmful to both mother and baby. For women trying to conceive, tobacco use makes it harder to become pregnant. Miscarriages are more likely in smokers, and there is an increase in the abortion rate by 33 percent. The risk of stillbirth increases by 23 percent in smokers. The risk of infections is higher in the unborn child if the mother is a smoker.

Smoking is associated with placental problems such as early separation from the womb (the placenta is the baby’s source of oxygen and nutrition). Maternal tobacco abuse can lead to the baby being born prematurely or having a low birth weight and health problems, requiring a more extended hospital stay. Maternal smoking is also a risk factor for SIDS (sudden infant death syndrome).
Alcohol Use
Alcohol use in expecting mothers is a widespread problem reported by 15 to 20 percent of women. More than 50 percent of women report drinking alcohol three months before conceiving. Nearly 7 percent of mothers report using alcohol during the last three months of their pregnancy. In women above the age of 30, the percentage of alcohol drinkers in the last trimester is higher at 10 percent.
The good news is that alcohol consumption by pregnant women seems to be on the decline. Effects of drugs and alcohol during pregnancy include many harmful consequences, including preterm labor. It is associated with a four times higher risk of spontaneous abortion. Fetal alcohol syndrome, a condition in which the baby suffers brain damage, malformations, and growth retardation, is a well-established consequence of maternal alcohol abuse and is present in 1 in 300 live births every year.
An estimated 2.6 million babies suffer in utero exposure to alcohol each year.
Marijuana Use
Over the past decade, there has been a significant increase in prenatal marijuana use from 4.2 percent to over 7 percent. Interestingly, the jump is even more substantial in women under 18, increasing from 12.5 percent to nearly 22 percent. The number of pregnant women seeking treatment for marijuana abuse has also increased. About 20 percent of pregnant women under 24 tested positive on drug testing for marijuana. Data from SAMHSA found that past-month marijuana use was reported by about 3.5 percent of pregnant females between the ages of 15 and 44. It would suggest a considerable gap between self-reported marijuana use in pregnant women and marijuana use discovered on drug screening tests. Medical experts warn against using marijuana to treat pregnancy-related nausea. Although recreational marijuana is legal in some states, women should not use it during pregnancy as it can lead to a low birth weight baby and behavioral problems such as hyperactivity later in life. In addition, long-term use of marijuana elevates the risk of premature birth. Women who use marijuana while pregnant have 2.3 times increased risk of stillbirth.
Caffeine
Caffeine is a stimulant and is present in tea, coffee, sodas, energy drinks, and some headache medications, in varying amounts. The data on maternal caffeine consumption and fetal safety are conflicting. What we do know is that pregnant women metabolize caffeine slower than non-pregnant women, and caffeine is transmitted across the placenta from the mother to the baby.

Studies suggest that one to two cups of coffee a day are safe. Still, intake of more than 300 mg per day may be associated with adverse outcomes such as spontaneous abortion, growth restriction, congenital malformations, and stillbirth. A typical 8-ounce serving of coffee has about 135 mg of caffeine. Studies have found that a 100 mg dose of caffeine per day from all sources is associated with an elevated risk of miscarriage. Research shows that high caffeine intake is associated with impaired fetal growth and low birth weight. There is a linear increase in risk. For every additional 100 mg of caffeine (1 cup of coffee or 2 cups of tea) per day, there is a 3 percent increase in low birth weight. Pregnant women who drink more than 8 cups of coffee a day are at increased risk of stillbirth. Fetal exposure to moderate to high levels of caffeine has been linked to childhood obesity.
Hallucinogens
Hallucinogens such as LSD, shrooms, and ecstasy alter a person’s perception of reality by causing them to see, hear, and feel things that are not real. It is difficult to establish a link between hallucinogens and adverse fetal outcomes because pregnant drug abusers often use other illicit substances simultaneously. One study found nearly 9 percent of women in the age group of 20 to 29 reported recent ecstasy use. There is no doubt that illicit substance abuse is associated with poor obstetric outcomes such as stillbirth and eclampsia.
Hallucinogen abuse while pregnant may increase the risk of miscarriage, premature delivery, and withdrawal symptoms in the newborn.
Babies born to mothers who abuse hallucinogens may have heart and brain abnormalities and be small in size. Studies show that spontaneous abortions occur significantly more frequently in mothers who use LSD. The drug can also lead to compromised fetal blood flow and ocular abnormalities in the baby. More research is needed to confirm whether LSD causes congenital disabilities.
Opioids
Drug use during pregnancy statistics is worrisome, especially when talking about opioids. According to the National Institute on Drug Abuse, 39 percent of women in the reproductive age group of 15-44 years enrolled in Medicaid have prescriptions written for narcotics, making opioid use in expecting mothers a major concern in America. There has been a dramatic increase in maternal opioid abuse in recent years, paralleling the epidemic in the general population. In some states, more than 41 percent of women reported filling a prescription for opioids when pregnant, with codeine and hydrocodone being the most commonly prescribed drugs.

Population-based studies by the CDC have found a link between the use of opioid painkillers by expectant mothers and birth defects in the baby. Maternal misuse of opioids is also associated with severe complications such as placental abruption, fetal growth retardation, preterm labor, and stillbirth. Abnormalities such as spina bifida, hydrocephalus, gastroschisis, glaucoma, and congenital heart defects are reported by pregnant women due to opioid painkiller use. Opioid use by the mother in the first trimester increases the chances of a heart defect in the baby by two times. It is estimated that every 25 minutes, a baby is born with neonatal abstinence syndrome (NAS), a type of drug withdrawal syndrome in newborns. In 2012, nearly 22,000 babies were born with NAS in the United States, representing a fivefold increase from the year 2000.
Stimulants (Cocaine and Methamphetamine)
It is estimated that approximately 4 percent of pregnant women are using drugs while pregnant. It is difficult to determine precisely how many expectant mothers use cocaine in the United States. A 2015 National Survey on Drug Use and Health found that approximately 1,000 expectant mothers had used cocaine in the preceding month. Despite the well-known fact that cocaine drug use during pregnancy has long-lasting harmful effects on both mother and baby, there are an estimated 750,000 cocaine-exposed pregnancies each year in the United States. Prenatal cocaine exposure is associated with several long-term health consequences and neurodevelopmental issues in the baby, including impaired language development and behavioral problems. Other adverse outcomes of cocaine abuse during pregnancy include preterm birth, placental problems, impaired fetal growth, congenital malformations, stillbirth, and SIDS (sudden infant death syndrome). Methamphetamine abuse during pregnancy is associated with placental abruption (separation of the placenta from the wall of the uterus). Infants born to mothers who abuse meth or cocaine may be hyperactive and irritable with excessive sucking, tremors, and high-pitched crying.
Amphetamines and Bath Salts
According to the World Health Organization, amphetamine-type stimulants are some of the most widely abused illicit drugs globally, making them highly likely to be abused by women of reproductive age. This is confirmed by the CDC finding that the percentage of American women in the reproductive age group who filled prescriptions for stimulant medications for ADHD treatment increased by 350 percent from 2003 to 2015. In addition, the hospitalization rate for amphetamine abuse during pregnancy doubled from 1998 to 2004. Unfortunately, there is not much research on the effects of amphetamine or bath salts drug use and pregnancy. What is known is that women abusing amphetamines and bath salts are at high risk of poor obstetric outcomes. Because the signs of amphetamine withdrawal are less pronounced than those of opiate withdrawal, this drug may remain undetected in some infants. The effects of bath salts during pregnancy are poorly understood but may include stillbirth, congenital malformations, and separation of the placenta. Low body weight, premature labor, and stillbirth are also reported. One study found that 35 percent of children exposed to amphetamines during fetal life exhibited aggressive behavior at four years of age.
Prescription Drugs During Pregnancy
In the United States, a woman seeks emergency care every 3 minutes for prescription drug abuse. In 2014, SAMHSA reported that 4.6 million women above 18 were misusing prescription drugs. The fast-growing abuse of prescription painkillers has not spared maternity wards. The number of babies born with prescription painkiller withdrawal symptoms has risen sharply over the past decade or so. Commonly abused prescription drugs include pain relievers such as Percocet, OxyContin, and Vicodin, CNS depressants such as Xanax, Valium, and Ativan, and stimulants such as Adderall and Ritalin. In the decade or so following the year 2000, there was a fivefold increase in opiate use during pregnancy. The risk of stillbirth is two to three times higher in women who take prescription pain relievers. About 13,500 babies are born with neonatal abstinence syndrome due to opiate withdrawal every year in the United States. Potential harm to the fetus includes low birth weight, preterm birth, and fetal death. Opiate exposure during fetal life can cause birth defects such as spina bifida and heart anomalies. Stimulants increase the risk of brain and heart defects and cleft palate or cleft lip in the baby.
Why Do Pregnant Women Use Cigarettes, Alcohol, and Drugs?
Most women, when they find out they are expecting a baby, do everything in their power to ensure a healthy birth. Yet, millions of babies continue to be exposed to harmful substances, including tobacco, alcohol, and drugs, while developing in their mother’s womb. What causes a mother to put her baby at risk? Why are there many women using drugs while pregnant?
Here Are Some of the Most Common Reasons for Drug Use During Pregnancy:
- AGE. Perhaps the biggest reason for substance abuse during pregnancy is that a woman’s reproductive years (age 15 to 44) coincide with a time in life when a person is most likely to seek out new experiences and begin abusing drugs. Adolescents and young adults are biologically wired to take risks and experiment with tobacco, alcohol, prescription pills, and illicit drugs. It puts women of childbearing age at an increased risk of addiction. Studies show that there is a higher percentage of pregnant teens abusing drugs than older women.
- UNPLANNED PREGNANCY. About 45 percent of pregnancies in the United States are unintended or mistimed, meaning either the pregnancy was not desired or occurred earlier than expected. Unplanned pregnancies are a risk factor for using drugs while pregnant due to late recognition of pregnancy and delayed access to antenatal care. When a pregnancy is unplanned, the woman may continue risky consumption of alcohol and drugs without realizing she is carrying a baby.
- PRESCRIPTION MEDICATIONS. Some of the drugs prescribed during pregnancy, such as benzodiazepines (sleeping pills), are highly addictive. In addition, prenatal exposure to benzos such as diazepam is associated with different adverse effects of drugs during pregnancy, like birth defects, including facial clefts and cardiac malformations. In pregnant women, treatment with any medication needs to be carefully monitored to ensure the mother does not become dependent and no harm is caused to the baby.
- INABILITY TO QUIT. Most women want to do what’s best for their babies. They realize that quitting tobacco, alcohol, or drugs is an essential step towards a healthy birth. Yet, changing behaviors is not easy. Not all women can stop smoking, drinking, or using drugs when they find out they are expecting, even if they are aware of the effects of drugs and alcohol during pregnancy. Daily smokers, heavy drinkers, and long-term drug abusers find it the hardest to quit. Studies show that only 1 in 3 women who smoked before pregnancy is able to quit in the prenatal period. Abstinence rates for alcohol and illicit drugs are slightly more encouraging, but relapse rates in the postpartum period remain high.
- UNDERESTIMATION OF RISK. Any chemical that enters a pregnant woman’s body, prescribed by a physician or used illegally for recreational purposes, can harm the fetus. However, not every expecting woman understands the risks of tobacco, alcohol, and drug abuse for herself and her baby. Some women are under the false impression that light drinking is okay, believing that only binge drinking is harmful to the baby. According to the CDC, no type or amount of alcohol is safe for pregnant women.
- FEAR OF CONSEQUENCES. It is mandatory for obstetricians to report substance abuse in pregnant women. Many expectant mothers are aware of drug use and pregnancy risks but avoid seeking treatment for their addiction because they are afraid of the legal ramifications. Some women fear being judged and criticized by friends, family, and healthcare providers. Some women are afraid they may lose custody of their children or be evicted from their homes if their addiction is discovered. The threat of institutionalization or incarceration keeps many pregnant women from seeking treatment for substance abuse.
- POSTPARTUM DEPRESSION. Pregnancy and the birth of a child are associated with many biological and lifestyle changes for a woman. Many women struggle to cope with and adapt to the new phase of their lives and suffer from depression. Postpartum depression, commonly known as baby blues, affects an estimated 15 percent of new mothers. Feelings of anxiety, sadness, and exhaustion make it difficult for the mother to care for herself and her baby. Studies show that women with postpartum depression are at a high risk of substance abuse. In fact, substance abuse and depression are risks for each other, and both have a substantial negative impact on maternal and infant health.
Dangers and Effects of Drugs and Alcohol During Pregnancy
It is well known that there are several serious health consequences for the developing fetus from maternal substance abuse. Some of the most common prenatal effects of drugs during pregnancy include miscarriage, preterm labor, low birth weight, and many developmental problems and birth defects. Pregnant women with addictions are a high-risk group that requires intensive obstetric and neonatal care. Let’s look at some of the most common adverse prenatal effects of tobacco, alcohol, prescription drugs, and illicit substances.
Neonatal Abstinence Syndrome (NAS)
A baby exposed to an illicit substance during fetal life because the mother was regularly using it can be born dependent on the substance. It is known as neonatal abstinence syndrome. Maternal abuse of drugs such as opioids (oxycodone, codeine), heroin, and methadone can cause NAS in a newborn infant. It can also be caused by exposure to alcohol, benzodiazepines (sleeping pills), and antidepressants (SSRIs) in the womb. Babies who receive one or more of these drugs before delivery from their mothers are born dependent on the drugs. After birth, when they no longer get the drugs, it results in a postnatal withdrawal syndrome.
The Symptoms Include:
- High-pitch crying
- Fever
- Excessive sucking
- Irritability
- Rapid breathing
- Vomiting
- Trembling
- Seizures
- Sleep problems
During the period 2000-2012, the incidence of NAS in the United States increased by 383 percent.
In 2013, 6 cases of NAS were reported per 1,000 births, up from 1.5 in 1999. Treatment for NAS often requires pharmacological intervention with medications such as methadone and morphine in up to 70 percent of infants. The treatment protocol can extend for several weeks, depending on the severity of the withdrawal, which in turn depends on the duration of in utero drug exposure.
Fetal Alcohol Spectrum Disorders (FASD)
Fetal alcohol spectrum disorders are a set of conditions that occur in babies that were exposed to alcohol during their mother’s pregnancy. FASD is characterized by growth problems and irreversible brain damage. The severity of fetal alcohol syndrome varies from child to child and depends on the duration and amount of maternal alcohol abuse.
One in 10 pregnant women reports alcohol use in the United States.
The CDC fact sheet on alcohol and pregnancy states that 3.3 million women in the United States are at risk of exposing their babies to alcohol.
Factors That Increase the Risk of FAS Include:
- Maternal age
- Poor socioeconomic status
- Heavy and frequent drinking
- A family history of alcoholism
In the 1980s and 1990s, the prevalence of FAS in America was estimated at 2 cases per 1,000 births. The CDC reports that assessment of school-going children has revealed a prevalence of 6 to 9 cases of FAS per 1,000 children. A recent study on more than 13,000 children in four U.S. communities found that fetal alcohol spectrum disorders are present in up to 5 percent of first graders.
Miscarriage and Stillbirth
Miscarriage is the death of a baby in the womb before 20 weeks of pregnancy. Stillbirth is the death of a baby in the womb after 20 weeks of pregnancy. There is a strong link between illicit drug use and stillbirth. According to the National Institutes of Health (NIH), smoking tobacco or marijuana, using illegal drugs, or misusing prescription painkillers during pregnancy increases the risk of stillbirth by two to threefold. Heavy alcohol use (more than three alcoholic drinks daily) during pregnancy increases the risk of spontaneous abortion by more than threefold.
Women who consume any amount of alcohol while pregnant have a 40 percent increased risk of stillbirth compared to women who do not drink at all.
As more and more states legalize recreational marijuana, the effects of this drug on the fetus are an increasing public health concern. The CDC estimates that 1 in 20 women in America uses marijuana while pregnant. Studies reveal that reducing illicit substances substantially reduces the risk of abortion.
Premature Labor and Birth
Any infant born before the 37th week of pregnancy (about three weeks before the due date) is considered premature. Premature infants have several problems, including low weight, breathing troubles, and difficulties with eating and drinking.
Prescription drug use during pregnancy may result in premature rupture of membranes. Babies born to mothers who abuse illicit drugs such as cocaine during pregnancy have a higher prematurity rate.

Women who consume seven or more alcoholic drinks per week while pregnant are more than three times likely to deliver prematurely.
Tobacco use during pregnancy raises the risk of premature birth. Besides active tobacco use, exposure to second-hand smoke during pregnancy is associated with a significantly higher rate of preterm delivery.
Developmental and Behavioral Problems
Many women who use alcohol or drugs during pregnancy are poly-substance abusers. Maternal substance abuse is closely linked to child development. Among the effects of drugs during pregnancy are many different physical, behavioral, developmental, cognitive, social, academic, and vocational problems.
According to one study, more than 30 percent of women who abused methamphetamines during pregnancy reported having a child with a physical or mental disability.
Prenatal marijuana use is associated with a significant increase in impulsiveness, hyperactivity, inattention, and delinquency in children aged 10. Prenatal exposure to MDMA and other recreational drugs is associated with poor mental and motor development in infants at one year of age. The severity of the disorder is heavily dose-dependent.
Keeping Baby Safe: Addiction Treatment During Pregnancy
Drug use during pregnancy statistics is not changing for the better. Without drug rehab, the health consequences for mother and child can be devastating. Substance abuse treatment can be hard, especially when the addiction is severe. The possibility of withdrawal symptoms may stop some women from getting therapy. However, it is the only way to ensure the baby’s safety and give birth to a completely healthy child.
Treatment programs for pregnant women can significantly benefit women struggling with addiction. Women should look for a treatment facility that offers a safe and supportive environment to help keep both the baby and the mother safe.
Drug Rehab During Pregnancy: Facts and Figures
According to a report by SAMHSA, about 5 percent of women between 15 and 44 who enter substance abuse treatment are pregnant at the time of admission. Among pregnant women seeking treatment at drug rehab centers, the number of women addicted to alcohol saw a decline from 2000 to 2010. Still, the number of women using drugs while pregnant increased from about 51 percent to nearly 64 percent, indicating that the substance of abuse reported at the time of rehab admission has changed over the years.
In the past couple of decades, prescription opioid overdose deaths in the United States increased dramatically by more than 500 percent. Mirroring this increase, the number of pregnant women admitted for treatment of prescription opioids as the primary substance of abuse increased from 2 percent in 1992 to 28 percent in 2012 despite the percentage of pregnant women seeking addiction treatment remaining more or less stable.
Drug Rehab in the First Trimester: Better Outcomes for Mother and Child
Effects of drugs during pregnancy are harmful and associated with poor outcomes for both mother and child. Women addicted to drugs or alcohol require specialized care, including prenatal care and addiction treatment, to address their complex medical and psychosocial needs. Studies have found that a comprehensive prenatal and addiction treatment program for women with alcohol or drug abuse history is associated with positive health outcomes. Women who contact the treatment center early in their pregnancy have the best outcome with a higher rate of breastfeeding and discharge home with the mother following delivery (as opposed to protective child custody or adoption). More than 90 percent of women who start addiction treatment care in the first trimester have custody of their baby at discharge.
Research shows that infants with only first-trimester exposure to methamphetamines fare better than infants with continuous exposure until the third trimester.
Studies have found that medication-assisted treatment with methadone therapy for opioid-addicted pregnant women is associated with reduced fetal morbidity, improved maternal health, and better prenatal care utilization.
Avoiding alcohol is recommended to all women who are pregnant or planning to become pregnant. Alcohol is most harmful to the developing fetus for the first 12 weeks of the pregnancy, but stopping drinking at any time, even during the second and third trimester, can help reduce risks. According to the CDC, brain development occurs throughout the pregnancy, and the sooner a pregnant woman stops drinking, the better it is for her and her baby.
Addiction Treatment In Pregnancy: Making the Best Choice
Getting help for addiction as early as possible in the pregnancy is beneficial to both mother and child. A comprehensive drug rehab program reduces the risk of miscarriage, preterm delivery, birth defects, and neonatal abstinence syndrome. It also restores the mother’s physical and psychological health to enable her to care for her baby during pregnancy and after birth.
According to a study published in the Journal of Substance Abuse, treatment outcomes are significantly improved for those enrolled in comprehensive residential substance abuse treatment programs for pregnant women and new mothers. Addiction in pregnancy is not the end of the road. It is possible to get help at drug rehab and save two lives in the process.
Hope Without Commitment
Find the best treatment options. Call our free and confidential helpline
Most private insurances accepted
Find Drug Rehabilitation Centers Near You Anywhere In the US
Addiction Resource team has compiled an extensive list of the top drug rehabilitation facilities around the country. Use our locator tool to find the best centers near you.
Page Sources
- National Addiction & HIV Data Archive Program, National Survey on Drug Use and Health, 2012. https://www.icpsr.umich.edu/icpsrweb/NAHDAP/studies/34933/version/3
- Kuczkowski, K. M. (2007). The effects of drug abuse on pregnancy. Current Opinion in Obstetrics and Gynecology, 19(6), 578-585. https://pubmed.ncbi.nlm.nih.gov/18007137/
- CDC, Cigarette Smoking During Pregnancy: United States, 2016. https://www.cdc.gov/nchs/products/databriefs/db305.htm
- Mund, M., Louwen, F., Klingelhoefer, D., & Gerber, A. (2013). Smoking and pregnancy—a review on the first major environmental risk factor of the unborn. International journal of environmental research and public health, 10(12), 6485-6499. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3881126/
- Bhuvaneswar, C. G., Chang, G., Epstein, L. A., & Stern, T. A. (2007). Alcohol use during pregnancy: prevalence and impact. Primary care companion to the Journal of clinical psychiatry, 9(6), 455. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2139915/
- Rasch, V. (2003). Cigarette, alcohol, and caffeine consumption: risk factors for spontaneous abortion. Acta obstetricia et gynecologica Scandinavica, 82(2), 182-188. https://pubmed.ncbi.nlm.nih.gov/12648183/
- Young-Wolff, K. C., Tucker, L. Y., Alexeeff, S., Armstrong, M. A., Conway, A., Weisner, C., & Goler, N. (2017). Trends in self-reported and biochemically tested marijuana use among pregnant females in California from 2009-2016. Jama, 318(24), 2490-2491. https://jamanetwork.com/journals/jama/article-abstract/2667052
- NIDA, Marijuana Research Report, Can marijuana use during and after pregnancy harm the baby? 2020. https://www.drugabuse.gov/publications/research-reports/marijuana/can-marijuana-use-during-pregnancy-harm-baby
- NIDA, Substance Use in Women Research Report, Substance Use While Pregnant and Breastfeeding, 2020. https://www.drugabuse.gov/publications/research-reports/substance-use-in-women/substance-use-while-pregnant-breastfeeding
- Morgan, S., Koren, G., & Bozzo, P. (2013). Is caffeine consumption safe during pregnancy?. Canadian Family Physician, 59(4), 361-362. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3625078/
- Bakker, R., Steegers, E. A., Obradov, A., Raat, H., Hofman, A., & Jaddoe, V. W. (2010). Maternal caffeine intake from coffee and tea, fetal growth, and the risks of adverse birth outcomes: the Generation R Study. The American journal of clinical nutrition, 91(6), 1691-1698. https://pubmed.ncbi.nlm.nih.gov/20427730/
- Scott, K., Fagermo, N., Callaway, L., & Lust, K. (2010). Illicit drug use in late pregnancy associated with stillbirth and eclampsia. Obstetric medicine, 3(3), 113-114. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4989590/
- Bhuvaneswar, C. G., Chang, G., Epstein, L. A., & Stern, T. A. (2008). Cocaine and opioid use during pregnancy: prevalence and management. Primary care companion to the Journal of clinical psychiatry, 10(1), 59. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2249829/
- NIDA, Methamphetamine Research Report What are the risks of methamphetamine misuse during pregnancy? 2020. https://www.drugabuse.gov/publications/research-reports/methamphetamine/what-are-risks-methamphetamine-misuse-during-pregnancy
- Patrick, S. W., Schumacher, R. E., Benneyworth, B. D., Krans, E. E., McAllister, J. M., & Davis, M. M. (2012). Neonatal abstinence syndrome and associated health care expenditures: United States, 2000-2009. Jama, 307(18), 1934-1940. https://jamanetwork.com/journals/jama/fullarticle/1151530
- NIMH, Perinatal Depression. https://www.nimh.nih.gov/health/publications/perinatal-depression
- May, P. A., Chambers, C. D., Kalberg, W. O., Zellner, J., Feldman, H., Buckley, D., ... & Hoyme, H. E. (2018). Prevalence of fetal alcohol spectrum disorders in 4 US communities. Jama, 319(5), 474-482. https://jamanetwork.com/journals/jama/article-abstract/2671465
- Khader, Y. S., Al-Akour, N., AlZubi, I. M., & Lataifeh, I. (2011). The association between second hand smoke and low birth weight and preterm delivery. Maternal and child health journal, 15(4), 453-459. https://pubmed.ncbi.nlm.nih.gov/20364365/
- Brecht, M. L., & Herbeck, D. M. (2014). Pregnancy and fetal loss reported by methamphetamine-using women. Substance abuse: research and treatment, 8, SART-S14125. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4011724/

 FindTreatment.gov
FindTreatment.gov