
 Edit by: Brittni
Edit by: Brittni
Suboxone addiction is misusing or becoming dependent on Suboxone, a prescription medication widely utilized in Medication-Assisted Treatment (MAT) for opioid addiction. Although Suboxone is effective in reducing opioid withdrawal symptoms and cravings, it leads to addiction when misused or taken without proper medical supervision. Suboxone addiction impairs both mental and physical health, making it important to identify early warning signs, understand the contributing risk factors, and explore effective treatment options. Data from the National Institute on Drug Abuse (NIDA) indicates that misuse of prescription drugs, including Suboxone, affects approximately 12.5 million Americans annually.
The common signs and symptoms of Suboxone addiction include increased cravings, building tolerance, and noticeable withdrawal symptoms when not taking the drug. Individuals struggling with Suboxone addiction exhibit behaviors such as frequent mood swings, inability to control drug use, and secretive actions related to substance use. Withdrawal symptoms, such as anxiety, muscle pain, nausea, and insomnia, are severe, leading many individuals to relapse without appropriate support. A study by Winstock AR, Lintzeris N, and Lea T. et al. 2011, titled “Should I stay or should I go? Coming off methadone and buprenorphine treatment,” revealed that 68% of patients reported overusing buprenorphine due to a fear of withdrawal symptoms. Cravings are a primary challenge in overcoming Suboxone addiction, as they trigger repeated use despite the negative consequences.
Table Of Contents:

Several risk factors that contribute to the likelihood of developing Suboxone addiction include a personal or family history of substance use disorders, mental health conditions, and exposure to environments where drug use is prevalent. Additionally, individuals who misuse Suboxone by taking higher doses or combining it with other substances are at an increased risk of developing dependency. Behavioral health conditions, such as depression and anxiety, also exacerbate the risk, as individuals use Suboxone to self-medicate without seeking proper treatment.
The side effects of Suboxone addiction include impaired cognitive function, strained relationships, financial instability, and reduced ability to maintain steady employment. Physiological effects such as respiratory issues and changes in brain chemistry persist with prolonged misuse. Furthermore, untreated Suboxone addiction leads to severe emotional consequences, including increased feelings of isolation, anxiety, and depression. These effects highlight the urgency of addressing Suboxone addiction through comprehensive treatment.
Effective Suboxone addiction treatment programs combine medication-assisted treatment with behavioral therapies and support groups to address the multifaceted nature of addiction. , as studied by Medscape in “Buprenorphine/Naloxone Toxicity Treatment & Management.” MAT has been shown to reduce relapse rates and improve recovery outcomes. Treatment options include behavioral health counseling and participation in support groups like Narcotics Anonymous (NA) or SMART Recovery. These approaches help individuals manage withdrawal symptoms, combat cravings, and rebuild healthy, drug-free lives. By integrating therapy, medical intervention, and peer support, recovery from Suboxone addiction becomes attainable, offering individuals the chance to regain control and stability.
What is Suboxone Addiction?
Suboxone addiction is a dependence on Suboxone, a prescription medication containing buprenorphine and naloxone, used for treating opioid addiction. While Suboxone helps individuals manage withdrawal symptoms and reduce opioid cravings, its misuse leads to physical dependence, psychological cravings, and abuse patterns. The addiction arises from using Suboxone in higher doses or outside medical supervision. Data from the National Institute on Drug Abuse (NIDA) indicates that misuse of prescription drugs, including Suboxone, affects approximately 12.5 million Americans annually.
Suboxone addiction is classified under Substance Use Disorder (SUD) in the DSM-5, specifically as a form of Opioid addiction if misuse involves opioids. The severity is determined by meeting 2-11 criteria, such as loss of control, continued use despite harm, and withdrawal symptoms. For Suboxone, unique indicators include intense cravings and withdrawal that lead to relapse.
A study by Samples H, Williams AR, Olfson M, Crystal S., et al. 2018, titled “Risk factors for discontinuation of Suboxone addiction treatment for opioid use disorders in a multi-state sample of Medicaid enrollees,” highlights significant challenges in Suboxone treatment retention, with over 28% of Medicaid patients discontinuing within the first month and 64.6% stopping before 180 days. Factors such as low initial doses, younger age, minority status, and comorbid substance use disorders contribute to difficulty in discontinuation, aligning with reports that 30% of Suboxone patients struggle to stop its use, underscoring its classification as a substance use disorder.
In the ICD-10, Suboxone addiction is classified under F11.2: Mental and Behavioral Disorders Due to Use of Opioids, Dependence Syndrome. This code encompasses the physical and psychological aspects of addiction, including tolerance, withdrawal, and compulsive use. Suboxone, due to its opioid partial agonist properties, falls within this broader opioid-related category, emphasizing the risks of dependence despite its therapeutic intent.
Suboxone addiction exhibits gender-specific patterns, with a study by Han B et al. 2021, titled “Trends in and Characteristics of Buprenorphine Misuse Among Adults in the US” showing that men are more likely to misuse Suboxone for its euphoric effects, whereas women are prescribed Suboxone to manage opioid addiction but face challenges with dependency due to physiological differences. It indicates that 62% of men report Suboxone misuse, compared to 38% of women, yet women report higher levels of stigma and difficulty accessing treatment. These disparities underscore the importance of gender-sensitive approaches in Suboxone addiction treatment.
Why is Suboxone Addictive?
Suboxone is addictive because it combines pharmacological and behavioral factors that contribute to dependency. As a partial opioid agonist, Suboxone contains buprenorphine, which binds to opioid receptors in the brain and produces mild euphoria, especially when misused at higher doses. While this mechanism is intended to prevent the intense highs of stronger opioids, it still activates the reward system enough to reinforce use. In the United States, buprenorphine is classed as a Schedule III controlled substance, meaning it has a low to moderate risk of physical or psychological dependence. Prolonged use leads to physical dependence, as the body becomes accustomed to its presence, making discontinuation difficult due to withdrawal symptoms such as agitation, muscle aches, and nausea, as studied by Medical News Today in “What to know about Suboxone addiction.” To avoid these symptoms, individuals continue using the drug, even if they wish to stop.
Over time, tolerance develops, requiring higher doses to achieve the same effect, which increases the risk of misuse. Additionally, Suboxone’s psychological impact has an addictive potential, as users develop cravings or rely on it to manage stress or emotional difficulties. These cravings persist even after the physical dependence has been addressed. Suboxone has a “ceiling effect,” meaning its effects plateau at a maximum dose of 24 milligrams per day, so taking higher doses doesn’t enhance its impact. This property, combined with its slow and steady action in the body, reduces the potential for misuse. While dependence on Suboxone occurs, its design makes addiction less likely, as explained by Healthline in “Can You Become Addicted to Suboxone? Separating Fact from Fiction.” Suboxone’s accessibility as a widely prescribed medication for opioid use disorder also contributes to its misuse potential, as some individuals obtain it illicitly.
The combination of partial opioid agonist effects, tolerance, withdrawal avoidance, psychological cravings, and ease of access creates a multifaceted risk of addiction. While Suboxone is an important tool in treating opioid use disorder, its potential for misuse and dependency requires vigilant monitoring and comprehensive care strategies.
What is Suboxone Used For?
Suboxone is primarily used for treating opioid use disorder (OUD) and managing withdrawal symptoms associated with opioid dependence. It combines buprenorphine, a partial opioid agonist, with naloxone, an opioid antagonist, to reduce cravings and withdrawal discomfort while minimizing the potential for misuse, as studied by Shulman M, Wai JM, and Nunes EV. et al. 2019, titled “Buprenorphine Treatment for Opioid Use Disorder: An Overview.” the study shows among all randomized patients, buprenorphine was modestly superior to XR-naltrexone on the primary outcome of relapse and the number of opioid-positive urines. The rate of relapse by the end of 24 weeks was 57% on buprenorphine versus 65% on injection naltrexone.
In opioid withdrawal management, Suboxone helps stabilize patients during the detoxification phase by alleviating severe symptoms. For ongoing OUD treatment, it is prescribed as part of a medication-assisted treatment (MAT) program, providing maintenance therapy to prevent relapse by reducing cravings without producing the euphoric effects of full opioid agonists like heroin or fentanyl. Suboxone also prevents relapse, allowing individuals to regain stability while participating in counseling or behavioral therapies. Its effectiveness and safety have been extensively validated, making it a cornerstone in addiction recovery programs.
How Common is Suboxone Addiction?
Suboxone addiction is relatively uncommon compared to other opioid-related substance use disorders due to its unique pharmacological properties, including its ceiling effect and inclusion of naloxone to deter misuse. However, cases of misuse and dependence have been reported, primarily among individuals with a history of substance use disorders.
In the United States, exact statistics on Suboxone addiction are limited, but studies indicate that about 2–5% of individuals prescribed Suboxone develop misuse behaviors, according to a study by Han B, Jones CM, Einstein EB, and Compton WM. et al. 2021, titled “Trends in and Characteristics of Buprenorphine Misuse Among Adults in the US.” Rates of misuse tend to vary across demographics, with younger adults and individuals in economically disadvantaged communities showing higher tendencies toward non-medical use. Racial disparities are less pronounced, but access to medication-assisted treatment, including Suboxone, remains unequal across racial groups, leading to differences in misuse patterns.
The death rate directly associated with Suboxone addiction remains low. In 2016, 67 deaths were associated with buprenorphine, and between 2013 and 2016, 10 Tennesseans died with only buprenorphine present, according to a study by the TN Department of Health in “TDH Finds Some Overdose Deaths Associated With Buprenorphine.” While Suboxone overdoses occur, especially when combined with other substances like benzodiazepines or alcohol, fatalities are rare due to the drug’s partial opioid agonist properties, which limit respiratory depression. Public health data suggest that Suboxone reduces opioid-related deaths by preventing relapse and supporting recovery efforts.
What is Suboxone?
Suboxone is a prescription medication primarily used to treat opioid use disorder (OUD) by reducing withdrawal symptoms and cravings. It is a combination drug containing buprenorphine and naloxone, which work together to manage addiction effectively. Buprenorphine is a partial opioid agonist, meaning it partially activates opioid receptors in the brain, producing enough opioid-like effects to alleviate withdrawal symptoms and cravings without causing the intense euphoria associated with full opioid agonists like heroin or oxycodone. This controlled activation helps stabilize patients during recovery.
Naloxone, on the other hand, is an opioid antagonist, which means it binds to opioid receptors but does not activate them, effectively blocking the effects of other opioids. When Suboxone is taken as prescribed (sublingually), naloxone remains inactive. However, if someone attempts to misuse Suboxone by injecting it, naloxone becomes active, triggering immediate withdrawal symptoms, thereby deterring misuse.
Suboxone is commonly available as a sublingual film or tablet that dissolves under the tongue for rapid absorption. Its unique mechanism of action—partially activating opioid receptors to manage symptoms while blocking misuse—makes it an effective tool for treating opioid addiction and supporting long-term recovery.
Is Suboxone a Controlled Substance?
Yes, Suboxone is a controlled substance. It is classified as a Schedule III drug under the Controlled Substances Act (CSA) in the United States. This classification indicates that Suboxone has a recognized medical use but also a moderate to low potential for physical and psychological dependence compared to drugs in Schedules I and II. It was reported that over 90% of buprenorphine prescriptions are for combined buprenorphine/naloxone, owing to the lower potential for misuse according to a study published by Cambridge University Press titled “Buprenorphine prescription, misuse and service provision: a global perspective.”
The primary component of Suboxone, buprenorphine, is a partial opioid agonist, which carries a risk of misuse and dependence, though it is significantly lower than that of full opioid agonists like heroin or oxycodone. A buprenorphine dose of 4 mg per day will bind approximately 50% of mu-opioid receptors, which is sufficient to suppress opioid withdrawal symptoms, according to a study by Togioka BM, Patel P. et al. 2024, tilted “Buprenorphine and Naloxone.” A buprenorphine dose of 16 mg will bind approximately 80% of mu-opioid receptors and is sufficient to block the euphoric effects of most abused opioids. To mitigate this risk, Suboxone also contains naloxone, an opioid antagonist that discourages misuse by causing withdrawal symptoms if injected. Despite these safeguards, misuse of Suboxone does occur, contributing to its status as a controlled substance.
Regulating Suboxone under Schedule III ensures that it is available for medical use while also being subject to monitoring and prescribing restrictions to minimize abuse. Healthcare providers must meet specific requirements and obtain certification to prescribe Suboxone under the Drug Addiction Treatment Act of 2000 (DATA 2000).
What are the Signs and Symptoms of Suboxone Addiction?
The signs and symptoms of Suboxone addiction include cravings, increased tolerance, and withdrawal symptoms, among others, spanning physical, cognitive, and psychosocial effects. Individuals struggling with Suboxone addiction exhibit a combination of these signs, reflecting the drug’s impact on both their body and behavior.
The main behavioral, physical, cognitive, and psychosocial signs of Suboxone addiction are explained below:
- Cravings: Cravings refer to an intense desire to use Suboxone, leading to obsessive thoughts about obtaining or consuming the drug. This psychological symptom is common among individuals with Suboxone addiction, as the brain’s reward pathways are altered over time. Two meta-analyses, one by Kennedy AJ et al. 2022, titled “Factors Associated with Long-Term Retention in Buprenorphine-Based Addiction Treatment Programs: a Systematic Review,” and another by Fareed A et al. 2012, titled “Effect of Buprenorphine dose on treatment outcome” found that the 16 mg/day to 32 mg/day dose was associated with greater treatment retention and a lower frequency of illicit opioid use compared to lower dosages. This is because higher doses of buprenorphine-naloxone are more effective at suppressing cravings than lower doses.
- Increased Tolerance: Tolerance occurs when an individual requires progressively larger doses of Suboxone to achieve the same effects. This physical symptom indicates that the body has adapted to the drug’s presence. Research by the National Institute of Health (NIH) shows that about 60% of individuals on long-term opioid therapy, including Suboxone, develop significant tolerance within six months.
- Withdrawal Symptoms: Withdrawal symptoms arise when a person reduces or stops Suboxone after prolonged use. These physical symptoms include sweating, nausea, muscle pain, and restlessness, reflecting the body’s dependence on the drug. Buprenorphine’s unique partial mu agonist pharmacology and extended receptor occupation time lend to a comparatively less severe withdrawal syndrome, as studied by Tompkins DA et al. 2013, in “A double-blind, within-subject comparison of spontaneous opioid withdrawal from buprenorphine versus morphine.” A less severe withdrawal syndrome could potentially reduce relapse propensity, a hypothesis supported by the observation that longer Opioid Maintenance Therapy tapering procedures result in better outcomes, according to Dunn KE et al. 2011, titled “The association between outpatient buprenorphine detoxification duration and clinical treatment outcomes: a review.”
- Drowsiness: Suboxone causes excessive drowsiness or sedation, particularly in higher doses. This physical symptom affects an individual’s ability to function during daily tasks, potentially impairing workplace or social performance. Suboxone slows brain function and causes sleepiness due to its central nervous system depressant effects. Buprenorphine, its primary ingredient, is an opioid known to promote relaxation and calmness by depressing the central nervous system. In clinical trials, 5% of patients reported sleepiness while using Suboxone, according to the study “Suboxone and Sleepiness: What You Need to Know” by Confident Health. However, not everyone experiences this side effect, as individual responses to the medication vary.
- Impaired Judgment: Suboxone addiction leads to impaired judgment, a cognitive symptom where decision-making and problem-solving abilities are compromised. This results in risky behaviors, including unsafe sexual practices or driving under the influence. Impaired judgment is reported in approximately 15-20% of Suboxone misuse cases (NIH, 2020).
- Financial Issues: The compulsion to obtain Suboxone leads to financial strain, as individuals spend excessive amounts of money to sustain their addiction. This behavioral symptom correlates with other signs, such as neglecting responsibilities. Research by the United Nations Office on Drugs and Crime (UNODC) highlights that financial difficulties are prevalent among the majority of individuals with substance use disorders. In a nationally representative survey in the USA, unemployment rates were 10.5% among those with an opioid use disorder compared with 3% of the general population and 7.1% for people with a non-opiate substance use disorder, as studied by Becker W.C., Fiellin D.A., Merrill J.O., et al. 2008, titled “Opioid use disorder in the United States: insurance status and treatment access.”
- Social Isolation: Addiction to Suboxone leads to withdrawal from social interactions, as individuals prioritize drug use over relationships. This psychosocial symptom contributes to loneliness and depression, further perpetuating addiction. Social isolation is associated with psychological states that are relevant to drug use, specifically depression. Depression is diagnosed in about 8% of the U.S. general population but is present in 25–30% of people who use opioids like buprenorphine, according to a study by Dinwiddie S.H., Reich T., Cloninger C.R. et al. 1992, titled “Psychiatric comorbidity and suicidality among intravenous drug users.”
- Neglecting Responsibilities: People addicted to Suboxone neglect their personal, professional, or family obligations, focusing solely on drug use. This behavioral symptom has lasting consequences on one’s life and relationships. People who use opioids have high rates of unemployment—as high as 87% in a ‘severely addicted’ population, according to a study by Segest E., Mygind O., Bay H., et al. 1990, titled “The influence of prolonged stable methadone maintenance treatment on mortality and employment: An 8-year follow-up.”
- Risky Behaviors: Engaging in risky behaviors, such as sharing needles or using Suboxone with other substances, is common among individuals with addiction. This behavioral sign increases the likelihood of adverse outcomes like infections or overdose. A 1997 meta-analysis by Harris E.C., Barraclough B. et al. 1997, titled “Suicide as an outcome for mental disorders,” found that there is a 14-fold increase in risk among people who use opioids.
- Doctor Shopping: Doctor shopping involves visiting multiple healthcare providers to obtain illicit prescriptions for Suboxone. This behavioral symptom is indicative of addiction severity and leads to legal consequences. According to the available literature, prevalence rates of doctor shopping vary widely, from 6.3% to 56%, with opioids having the highest rate of 12.8%, according to a study by Wilsey BL, Fishman SM, Gilson AM, et al. 2010, titled “Profiling multiple provider prescribing of opioids, benzodiazepines, stimulants, and anorectics.”
What are the Causes of Suboxone Addiction?
The common causes of Suboxone addiction include misuse, overprescription, and self-medication, among other factors. These causes interplay with environmental, psychological, genetic, and social aspects, increasing the likelihood of addiction. Individuals with a history of substance use disorders or untreated emotional trauma are at a higher risk of developing dependency.
The main risk factors of Suboxone addiction are explained below:
- Misuse: Suboxone misuse, such as taking higher doses or using it without a prescription, leads to addiction. Its euphoric effects, although limited, encourage non-prescribed use. A study by Auriacombe M et al. 2004, titled “French field experience with buprenorphine,” estimates that up to 20% of Suboxone users misuse the drug at some point, increasing their risk of dependency.
- Overprescription: Excessive or prolonged prescribing of Suboxone for opioid use disorder (OUD) contributes to addiction. While intended for tapering off opioids, some individuals develop dependency due to extended treatment durations. Research by Samples H et al. 2020, titled “Impact Of Long-Term Buprenorphine Treatment On Adverse Health Care Outcomes In Medicaid,” indicates that nearly 15% of patients on long-term Suboxone therapy report addiction-like behaviors.
- Self-Medication: People turn to Suboxone for self-medicating chronic pain, anxiety, or depression, especially if professional care is unavailable. This psychological factor encourages reliance on the drug to manage distress. In the quantitative study by Richert, T., Johnson, B. et al. 2015, titled “Long-term self-treatment with methadone or buprenorphine as a response to barriers to opioid substitution treatment: the case of Sweden,” 32% of the interviewees stated self-treatment with Buprenorphine as their primary motive for illicit use leading to addiction.
- Dependency: Suboxone’s partial opioid agonist properties cause physical and psychological dependence with prolonged use. Dependency manifests in tolerance and withdrawal symptoms, perpetuating addiction. Nearly half of those using Suboxone for OUD treatment develop some level of dependence, according to a study by Kumar R et al. 2024 in their research titled “Buprenorphine.”
- Polysubstance Use: Combining Suboxone with other substances, such as alcohol or sedatives, heightens addiction risks by altering brain chemistry. Polysubstance use complicates treatment and withdrawal. A study by Saloner B et al. 2021, titled “Polysubstance Use Among Patients Treated With Buprenorphine From a National Urine Drug Test Database,” found that among 150,000 patients whose urine drug test (UDT) specimens were analyzed, 47.58% tested positive for at least one nonprescribed substance despite 85.49% of specimens being positive for buprenorphine.
- Accessibility: The relative ease of obtaining Suboxone, legally or illegally, contributes to its misuse. Increased access through online pharmacies and unregulated channels has raised concerns. In 2021, 15% of surveyed Suboxone users reported obtaining it without a prescription, as reported by SAMHSA.
- Withdrawal Avoidance: Suboxone’s ability to stave off withdrawal symptoms from other opioids leads to prolonged and unsupervised use, leading to addiction. A study by Winstock AR, Lintzeris N, and Lea T. et al. 2011, titled “Should I stay or should I go? Coming off methadone and buprenorphine treatment,” revealed that 68% of patients reported overusing buprenorphine due to a fear of withdrawal symptoms.
- Psychological Stress: Stressors such as job loss, financial difficulties, or personal conflicts drive individuals to misuse Suboxone as a coping mechanism. Psychological stress is a major risk factor implicated in 35% of addiction cases, as studied by the American Psychological Association (APA) in 2021.
- Peer Influence: Social factors, including peer pressure and normalization of Suboxone misuse, significantly contribute to addiction, particularly among younger populations. A study by Watts, L.L., Hamza, E.A., Bedewy, D.A. et al. 2024, titled “A meta-analysis study on peer influence and adolescent substance use,” reveals that nearly 20% of adolescents and young adults misuse Suboxone under peer influence.
- Chronic Pain: People with chronic pain misuse Suboxone for its analgesic effects, leading to dependency. This issue is especially prevalent among individuals without proper pain management alternatives. According to a PubMed study, the rate of opioid misuse among chronic pain patients is between 21% and 29%, according to a survey by Vowles KE et al. 2015, titled “Rates of opioid misuse, abuse, and addiction in chronic pain: a systematic review and data synthesis.” The rate of addiction is noted to be between 8% and 12%.
- Lack of Education: Limited awareness about Suboxone’s addictive potential and safe use practices lead to unintentional misuse. Many individuals start using Suboxone without fully understanding its risks, including its potential to cause dependence when not taken as prescribed. This lack of education stems from insufficient patient counseling and a broader misunderstanding of the medication’s role in treatment.
- Emotional Trauma: Past emotional trauma, such as abuse or neglect, predisposes individuals to addiction as they seek relief through substances like Suboxone. A study by Farrugia PL et al. 2010, titled “Childhood trauma among individuals with co-morbid substance use and post-traumatic stress disorder,” found that 75% of people with Substance Use Disorder, including Suboxone have experienced trauma in their lives, and up to 95% of people seeking treatment for addiction have a history of trauma exposure.
- Genetic Predisposition: Genetic factors significantly influence addiction risks, with certain inherited traits affecting how individuals respond to Suboxone. About 40% to 60% of addiction vulnerability is linked to genetic predisposition, as studied by Learn Genetics in “Genes and Addiction.”
- Environmental Factors: Environmental influences, such as living in areas with high drug misuse rates or exposure to substance-using peers, increase addiction risks. A study by Mennis J, Stahler GJ, Mason MJ, et al. 2016, titled “Risky Substance Use Environments and Addiction: A New Frontier for Environmental Justice Research,” highlights how environmental factors, such as community resources, socioeconomic conditions, and exposure to high-risk areas, significantly contribute to addiction.
Can you Overdose on Suboxone?
Yes, you can overdose on Suboxone, though the risk is lower compared to full opioid agonists due to its ceiling effect. Suboxone contains buprenorphine, a partial opioid agonist, and naloxone, an opioid antagonist, which together limit the drug’s euphoric potential and respiratory depression. However, overdose still occurs, particularly when Suboxone is combined with other central nervous system depressants such as benzodiazepines or alcohol. A study by Tracqui A., Kintz P., and Ludes B. et al. 1998, titled “Buprenorphine-related deaths among drug addicts in France: a report on 20 fatalities,” highlights that fatal overdoses involving Suboxone (buprenorphine) are rare but occur, particularly in cases of misuse. Over 16 months, 20 fatalities were documented in France, primarily involving intravenous injection of crushed buprenorphine tablets and co-use of psychotropics like benzodiazepines. The blood levels of buprenorphine in these cases fell within or slightly above the therapeutic range, suggesting that improper administration and combining substances significantly increase overdose risk.
Symptoms of Suboxone overdose include extreme drowsiness, respiratory depression, confusion, and loss of consciousness. According to the Substance Abuse and Mental Health Services Administration (SAMHSA), combining Suboxone with other sedatives increases the risk of life-threatening side effects. While the medication is designed to reduce misuse, improper use still leads to overdose.
What are the Side Effects of Suboxone Addiction?
The common side effects of Suboxone addiction include cravings, drowsiness, and nausea. These side effects represent the physical, psychological, and social challenges faced by individuals struggling with Suboxone addiction, and their severity varies based on the extent of misuse and individual factors
The common side effects of Suboxone addiction are as follows:
- Cravings: Cravings are intense urges to use Suboxone despite the negative consequences. These psychological side effects arise from the brain’s dependence on the drug for dopamine release, leading to compulsive behaviors. Cravings persist for months or years without proper treatment, making them a long-term challenge for recovery. Tiffany ST, Wray JM. et al. 2012, in their study titled “The clinical significance of drug craving,” suggest that cravings occur in a significant number of individuals with substance use disorders, contributing significantly to relapse risks.
- Drowsiness: Drowsiness occurs as a result of Suboxone’s effects as a partial opioid agonist, which slows central nervous system activity. This physical side effect impairs daily functioning and creates hazards, such as increased risks of accidents. Drowsiness is short-term, but chronic misuse exacerbates the symptom, affecting overall quality of life. Buprenorphine/naloxone causes drowsiness, particularly when taken together with alcohol or central nervous system depressants, as studied by Drugs.com.
- Nausea: Nausea is a common gastrointestinal side effect resulting from Suboxone’s impact on the opioid receptors in the digestive system. This physical effect is usually short-term but persists in cases of prolonged misuse. Medical News Today estimates that around 15% of Suboxone users report nausea as a side effect during initial treatment phases.
- Depression: Depression is a psychological side effect linked to Suboxone addiction, stemming from its impact on brain chemistry and the individual’s emotional health. Depression ranges from mild to severe and persists long-term, requiring therapy and medication for management. In a study by Bastien G. et al. 2021, titled “Preferences for research design and treatment of comorbid depression among patients with an opioid use disorder: A cross-sectional discrete choice experiment,” up to 74 % of people with any type of opioid use disorder (OUD) will experience depression in their lifetime.
- Impaired Cognition: Suboxone addiction leads to impaired cognition, affecting memory, decision-making, and problem-solving abilities. This neurological side effect is linked to the drug’s depressive effects on the central nervous system and worsens with long-term use. Impaired cognition significantly impacts work and social interactions, contributing to broader life challenges.
- Constipation: Constipation occurs as Suboxone slows intestinal motility, a common side effect of buprenorphine. This physical symptom is mild but becomes severe with prolonged addiction, potentially leading to serious gastrointestinal complications. A study conducted on a representative sample of 15,213 individuals in France by Ducrotté P et al. 2017, titled “Prevalence and clinical features of opioid-induced constipation in the general population: A French study of 15,000 individuals,” found that 31.2% reported opioid use in the past six months, with 8.7% experiencing opioid-induced constipation (OIC). The prevalence of OIC increased to 21% among individuals using opioids regularly or for more than one month. Factors associated with higher OIC rates included female gender, age ≥50 years, and use of step III opioids like buprenorphine.
- Respiratory Issues: Respiratory issues develop as Suboxone suppresses the respiratory system, particularly when combined with other depressants like alcohol or benzodiazepines. These physical side effects are life-threatening and are a significant concern in overdose cases. Respiratory depression is one of the leading causes of opioid-related fatalities, according To A Study By Pfizer In “Serious and Life-Threatening Risks From Use of Buprenorphine Hydrochloride Injection.”
- Apathy: Apathy, or lack of interest in daily activities, is a psychological effect of Suboxone addiction. It stems from the drug’s impact on dopamine regulation, leading to reduced motivation and emotional numbness. This symptom hinders recovery efforts and worsens social and professional relationships.
- Relationship Strain: Relationship strain arises from behavioral changes associated with Suboxone addiction, such as secrecy, irritability, or neglect of responsibilities. This social side effect leads to isolation, family conflict, or loss of social support, complicating recovery, as studied by Lander L, Howsare J, Byrne M., et al. 2013, titled “The impact of substance use disorders on families and children: from theory to practice.”
- Financial Problems: Financial problems are common in Suboxone addiction due to the cost of obtaining the drug, particularly when misused. This behavioral side effect leads to debt, job loss, or legal troubles, further perpetuating the cycle of addiction.
- Risky Behavior: Risky behavior includes actions like driving under the influence or engaging in illegal activities to obtain Suboxone. This behavioral symptom significantly increases the chances of accidents, injuries, or legal consequences.
- Tolerance: Tolerance develops as the body becomes accustomed to Suboxone, requiring higher doses to achieve the same effects. This physical side effect is a key marker of addiction, as it leads to increased misuse and potential overdose.
- Dependence: Dependence occurs when the body adapts to Suboxone use, leading to withdrawal symptoms upon cessation. This physical and psychological side effect is a defining characteristic of addiction, making it difficult for individuals to quit without medical assistance.
- Isolation: Isolation is a psychosocial symptom of Suboxone addiction, driven by shame, secrecy, or strained relationships. It exacerbates feelings of loneliness and hinders access to support systems necessary for recovery.
- Legal Issues: Legal issues arise from behaviors like doctor shopping, forging prescriptions, or possession of illicit Suboxone. These behavioral side effects can lead to criminal charges, imprisonment, or other severe consequences, impacting an individual’s future prospects.
How Does Suboxone Affect the Brain?
Suboxone affects the brain by interacting with its opioid receptors, primarily targeting the mu-opioid receptor. As a partial opioid agonist, buprenorphine, a key component of Suboxone, activates these receptors but to a lesser extent than full agonists like heroin or morphine. This produces a controlled effect, helping to alleviate withdrawal symptoms and reduce cravings without the intense euphoria linked to other opioids. The naloxone in Suboxone acts as an opioid antagonist, discouraging misuse by causing withdrawal symptoms if the medication is injected rather than taken as prescribed.
Over time, Suboxone alters brain chemistry by stabilizing disrupted opioid receptor function, which supports recovery from opioid addiction, as studied by Bicycle Health in “How Does Buprenorphine Work in the Brain?” However, prolonged use also leads to physical dependence as the brain adapts to its presence. Discontinuation results in withdrawal symptoms, highlighting its impact on neural pathways associated with pain, mood regulation, and reward. Suboxone’s effects on the brain are integral to its role in managing opioid use disorder, offering therapeutic benefits while posing risks of dependence if not used correctly.
How Does Suboxone Affect the Body?
Suboxone affects the body by providing a controlled level of opioid activity, reducing the physical symptoms of opioid withdrawal and dependence, as studied by Bicycle Health in “How Does Buprenorphine Work in the Body?” Buprenorphine helps stabilize bodily functions disrupted by opioid addiction, such as respiration and gastrointestinal activity while minimizing the risk of overdose due to its “ceiling effect.” Naloxone prevents misuse and adds a safeguard against respiratory depression. Over time, Suboxone use causes side effects like drowsiness, constipation, and hormonal imbalances. When used under medical supervision, it supports recovery by helping to restore the physical equilibrium disrupted by opioid abuse.
How Does Suboxone Addiction Affect Women Differently Than Men?
Suboxone addiction affects women differently than men due to variations in biological, psychological, and social factors. Women are more likely to experience intensified withdrawal symptoms and cravings, as hormonal fluctuations, especially during menstrual cycles, influence opioid sensitivity and dependence. Women progress more quickly from initial opioid use to addiction, a phenomenon known as “telescoping.” A higher CYP3A4 activity in women influences drug metabolism rates. Women are more likely to misuse benzodiazepines alongside buprenorphine, increasing overdose risks. Additionally, women have a higher predisposition to cardiac complications like QT interval prolongation due to hormonal effects on heart electrophysiology. A study by Unger A, Jung E, Winklbaur B, Fischer G., et al. 2010, titled “Gender issues in the pharmacotherapy of opioid-addicted women: buprenorphine,” also indicates that while buprenorphine is associated with fewer neonatal complications compared to methadone, women experience greater challenges during induction and unique withdrawal risks in pregnancy.
Secondary differences include higher rates of co-occurring mental health conditions such as anxiety and depression among women, which exacerbate addiction severity. Women are also more likely to face social stigma related to addiction, potentially leading to delayed treatment. Conversely, men exhibit riskier behaviors like polysubstance use, which complicate addiction management. Women respond more positively to behavioral interventions, as evidenced by greater clinical improvements in symptoms, mental health, and activity levels with collaborative care (CC), along with higher engagement and perceived benefits from psychotherapy, according to a study by Grubbs KM et al. 2015, titled “The role of gender in moderating treatment outcome in collaborative care for anxiety.” In contrast, men showed no significant differences between CC and usual care, suggesting they benefit more from medication-focused treatments. These gender-specific dynamics underscore the importance of tailored approaches to Suboxone addiction treatment for optimal outcomes.
How to Diagnose Suboxone Addiction?
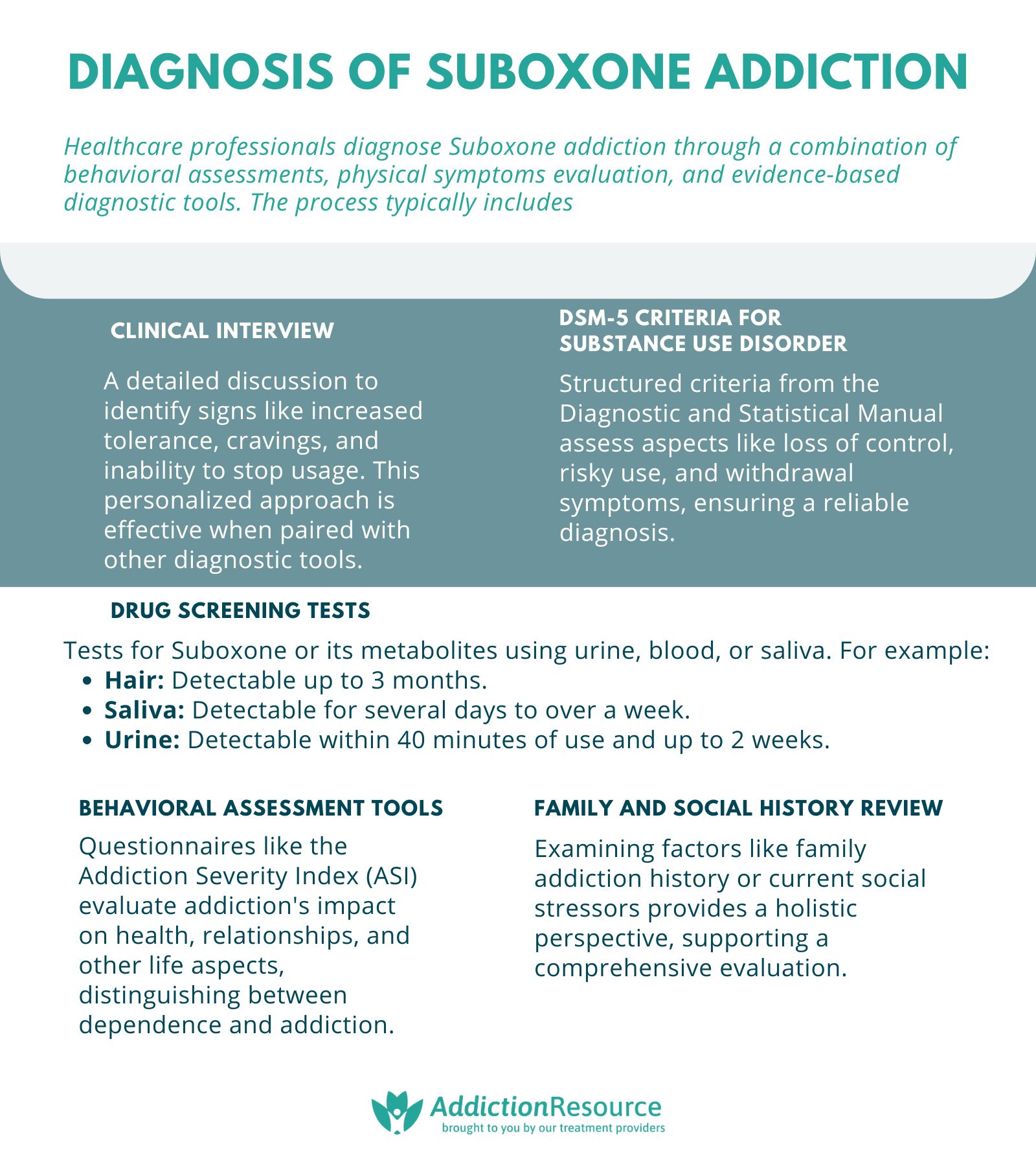
To diagnose Suboxone addiction, healthcare professionals assess behavioral patterns physical symptoms, and conduct evaluations using evidence-based diagnostic tools. The process involves thorough interviews, medical history reviews, and, when necessary, diagnostic tests to confirm dependence or misuse.
To diagnose Suboxone addiction, the following methods are employed:
- Clinical Interview: The clinical interview involves a detailed discussion between the patient and a healthcare provider to identify signs of Suboxone misuse, including increased tolerance, cravings, and difficulty in stopping usage. This method provides context-specific insights and is highly effective when combined with other diagnostic tools.
- DSM-5 Criteria for Substance Use Disorder: This method uses the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) to evaluate criteria like loss of control, risky use, and withdrawal symptoms. It offers a structured framework with high reliability that is commonly used in addiction diagnosis.
- Drug Screening Tests: Urine, blood, or saliva tests detect Suboxone levels or its metabolites. These tests provide objective evidence of use, especially useful in cases of suspected misuse or when patients underreport usage. However, they are complementary to behavioral assessments rather than standalone. According to Drugs.com, Suboxone is detectable in the body for varying durations depending on the testing method: up to 3 months in hair, a few days to more than a week in saliva, and up to 2 weeks in urine. Buprenorphine, the active ingredient in Suboxone, becomes detectable in urine as quickly as 40 minutes after consumption, making urine tests effective for early detection.
- Behavioral Assessment Tools: Questionnaires like the Addiction Severity Index (ASI) measure the impact of addiction on various life areas, including health and relationships. These tools provide a comprehensive picture, helping differentiate between dependence and addiction.
- Family and Social History Review: Reviewing a patient’s background, including family history of addiction or current social stressors, helps identify contributing factors to Suboxone misuse. This holistic approach supplements other diagnostic methods, ensuring a well-rounded assessment.
What Tests Are Used to Diagnose Suboxone Addiction?
The tests that are used to diagnose Suboxone addiction include urine tests, blood tests, saliva tests, and hair follicle tests. A 12-panel urine test is the most common method for screening Suboxone use, as it detects buprenorphine within 40 minutes of consumption and remains accurate for up to two weeks after the last dose, according to a study by Drugs.com. These tests are practical for routine screening and have a high accuracy rate for detecting recent use. According to Halux Diagnostics, urine testing is the most reliable form of drug testing, with an accuracy rate of over 99%.
Blood tests are highly accurate for detecting Suboxone use within 24 hours, as they directly measure the drug’s presence in the bloodstream. However, they are limited by a short detection window and their requirement for specialized lab equipment. Saliva tests are non-invasive, making them more comfortable for the patient, and detect buprenorphine use for a few days up to a week after ingestion. They are reliable but less accurate than blood tests for detecting very recent or low-dose use.
Hair follicle tests provide the longest detection window, identifying buprenorphine use for up to three months after consumption. According to the Università di Torino study, “Hair analysis for long-term monitoring of buprenorphine intake in opiate withdrawal,” all hair samples showed buprenorphine (BUP) concentrations higher than 10 pg/mg, even at the lowest dosage levels. Combining these methods improves overall diagnostic accuracy.
How to Treat Suboxone Addiction?
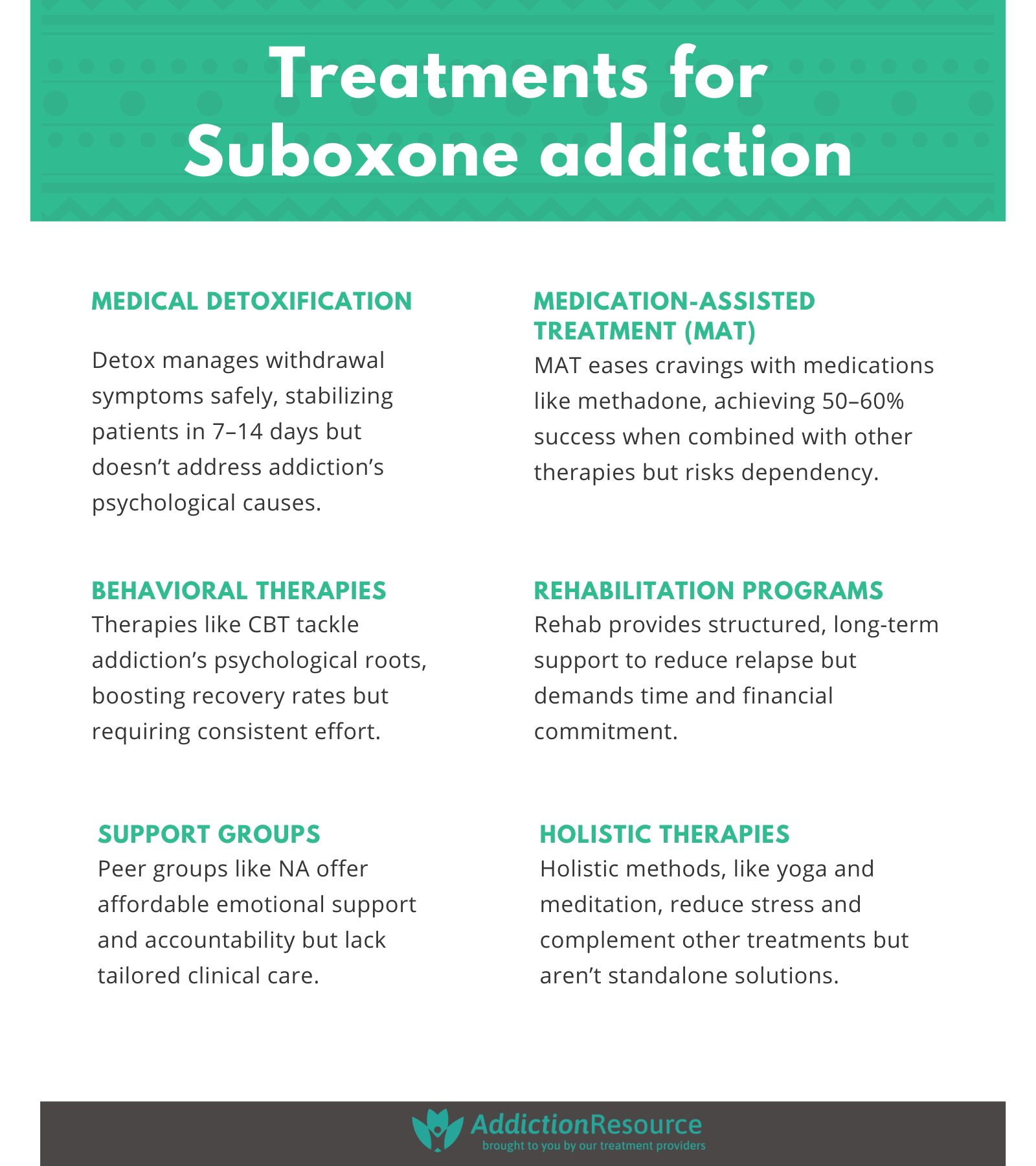
To treat Suboxone addiction effectively, a comprehensive approach involving multiple treatment methods is required. These methods include medical detoxification and withdrawal management, medications, behavioral therapies, long-term rehabilitation programs, and support groups. Each approach offers unique advantages and has varying success rates based on individual circumstances. Combining treatments such as MAT with behavioral therapies and support groups has proven most effective, with up to 68% recovery rates reported by the Substance Abuse and Mental Health Administration (SAMHSA) when employing a comprehensive, multidisciplinary approach.
The main treatments for Suboxone addiction are explained below:
- Medical Detoxification and Withdrawal Management: Medical detoxification involves supervised withdrawal under medical supervision to ensure safety and minimize discomfort from withdrawal symptoms. This is usually the first step in the recovery journey, focusing on stabilizing patients and managing acute withdrawal symptoms. Withdrawal symptoms from Suboxone include nausea, vomiting, anxiety, and muscle pain. Medical detoxification is effective in reducing relapse rates when combined with other treatments. The average detox program lasts about 7-14 days, according to the National Institute on Drug Abuse. While effective in addressing physical dependence, withdrawal alone does not address underlying psychological triggers, according to a study by Diaper AM, Law FD, Melichar JK. et al. 2014, titled “Pharmacological strategies for detoxification.”
- Medications (Medication-Assisted Treatment or MAT): Medication-assisted treatment (MAT) uses FDA-approved medications to manage withdrawal symptoms and cravings associated with Suboxone addiction. Common medications include methadone and naltrexone. If administered in single-dose increments, high doses of naloxone (up to 10 mg) are needed to reverse the clinical effects of buprenorphine. If naloxone does not reverse clinical effects, supportive ventilatory care must continue, as Medscape studied in “Buprenorphine/Naloxone Toxicity Treatment & Management.” MAT has been shown to reduce relapse rates and improve recovery outcomes. According to the Substance Abuse and Mental Health Services Administration (SAMHSA), MAT achieves an approximate 50-60% success rate when utilized in combination with other treatment methods. The advantages include reduced withdrawal symptoms and increased treatment adherence, but disadvantages include the potential for misuse or dependency on the medications themselves.
- Behavioral Therapies: Behavioral therapy focuses on addressing the psychological aspects of addiction, helping individuals recognize and change harmful behaviors or thought patterns, according to a study by Durpoix A, Rolling J, Coutelle R, Lalanne L., et al. 2024, titled “Psychotherapies in opioid use disorder: toward a step-care model.” Types of therapies include Cognitive Behavioral Therapy (CBT), Motivational Interviewing (MI), and Contingency Management (CM). Behavioral therapies have been effective in addressing triggers for relapse and improving coping mechanisms. A study by McHugh RK, Hearon BA, Otto MW. et al. 2010, titled “Cognitive behavioral therapy for substance use disorders,” show that behavioral therapies can increase abstinence rates by up to 40-50%. These therapies are highly personalized and combined with MAT for more effective results. While highly effective, the main disadvantage is the need for ongoing commitment and time investment from the patient.
- Long-Term Rehabilitation Programs: Rehabilitation programs involve structured, long-term residential or outpatient treatment focused on addressing addiction through education, counseling, therapy, and skill-building. These programs last between 30 days to 6 months or longer, depending on individual needs. Long-term programs offer a structured, drug-free environment that reduces the likelihood of relapse but requires the patient to stay in the facility for at least 30 days. According to the Substance Abuse and Mental Health Services Administration (SAMHSA), long-term rehabilitation programs achieve recovery success rates of 30-60%. They are especially effective because they focus on both physical and psychological aspects of addiction recovery. However, they are costly and require full commitment from the individual. In contrast, Intensive Outpatient Programs (IOPs) is a flexible and structured treatment option for Suboxone addiction, combining behavioral therapies, individual counseling, group therapy, and Medication-Assisted Treatment (MAT) to address both psychological and physical dependence. These programs require participants to attend 3–5 sessions per week while living at home, offering a success rate of 50–60% when fully engaged, according to a study by McCarty D, Braude L et al. 2014, titled “Substance abuse intensive outpatient programs: assessing the evidence.” Advantages of IOP include affordability, personalized care, and the ability to maintain work and family commitments, while disadvantages involve the need for high motivation, the risk of relapse due to less supervision, and time commitments.
- Support Groups: Support groups, such as Narcotics Anonymous (NA) or SMART Recovery, are peer-led initiatives that provide emotional support and shared experiences for individuals in recovery. These groups encourage community, reduce isolation, and provide motivation by connecting participants with others who are facing similar struggles. Participation in support groups improves the likelihood of long-term recovery, with success rates varying from 30-50%, as studied by Tracy K Wallace SP. et al. 2016, in “Benefits of peer support groups in the treatment of addiction.” Support groups are advantageous because they are accessible affordable, and encourage a sense of accountability and shared understanding. However, they lack the individualized treatment aspects that clinical therapies provide.
- Holistic and Alternative Therapies: Holistic therapies focus on treating addiction through non-conventional means, incorporating practices like yoga, meditation, acupuncture, nutritional therapy, and mindfulness. While evidence supporting holistic therapies remains limited, some studies suggest they reduce stress and improve mental well-being, thus supporting recovery goals, like a review of 8 randomized controlled trials (RCTs) on yoga as a treatment for substance use disorders conducted by Walia N et al. 2021, titled “Yoga for Substance Use: A Systematic Review,” found that 7 out of 8 studies showed significant improvements in primary outcomes such as anxiety, pain, and cravings, with a success rate of 87.5%. According to the Journal of Substance Abuse Treatment, these holistic therapies improve recovery outcomes when paired with conventional treatments, although they are not a standalone solution. Combining yoga with pharmacological treatments like opioid substitution therapy enhanced positive outcomes, as claimed by Walia N et al. 2021, although larger studies are needed to confirm its effectiveness fully. The recovery timeline depends on the individual’s commitment to these therapies, but they complement MAT or behavioral therapies effectively.
What is Suboxone Tolerance?
Suboxone tolerance is the gradual reduction in the drug’s effectiveness, requiring increased doses to achieve the same therapeutic effect. Tolerance develops as the body becomes accustomed to the presence of Suboxone, primarily due to the drug’s mechanism of action. Suboxone, which combines buprenorphine (a partial opioid agonist) and naloxone (an opioid antagonist), binds to opioid receptors in the brain to relieve withdrawal symptoms and cravings. Over time, repeated use leads to receptor desensitization, meaning the opioid receptors become less responsive, thus reducing Suboxone’s efficacy. This process differs from dependence, as tolerance focuses on the diminished effect of the drug rather than the body’s adaptation to avoid withdrawal symptoms. Tolerance develops with long-term use, and higher doses become necessary for continued relief.
What is Suboxone Dependence?
Suboxone dependence is the physiological adaptation of the body to the presence of Suboxone, characterized by the need to continue taking the drug to avoid withdrawal symptoms. Dependence occurs as the brain and body adjust to the presence of buprenorphine and naloxone, leading to a state where the drug must be taken regularly to maintain normal functioning. It differs from addiction, which involves a psychological and behavioral compulsion to seek out Suboxone regardless of its medical necessity or adverse consequences. While dependence occurs naturally during therapeutic use for opioid use disorder treatment, addiction involves more than physical reliance and includes cravings, loss of control, and compulsive drug-seeking behavior. While Suboxone helps manage opioid withdrawal and cravings, dependence develops, necessitating careful management under medical supervision to avoid misuse.
What Withdrawal Symptoms are Associated with Suboxone Addiction?
The withdrawal symptoms that are associated with Suboxone addiction include anxiety, muscle pain, and nausea. Anxiety is one of the most common symptoms during Suboxone withdrawal, affecting up to 50% of patients undergoing treatment due to the sudden decrease in opioid receptor stimulation, according to Medical News Today. Muscle pain is another prevalent symptom, stemming from the body’s adaptation to the absence of buprenorphine’s opioid effects, leading to severe discomfort and reduced physical function. Nausea and vomiting are also frequently reported, impacting approximately 15% of Suboxone users as a side effect during initial treatment phases. These symptoms drastically impair daily life by limiting physical and psychological functionality, contributing to intense cravings and emotional distress. The physiological cause of these symptoms is primarily rooted in the action of buprenorphine, a partial opioid agonist, which modulates opioid receptor activity. Upon discontinuation or reduction of Suboxone, the body’s lack of opioid receptor stimulation triggers these physical and psychological withdrawal responses, making recovery challenging without proper medical oversight.
What is the Withdrawal Timeline for Suboxone?
The withdrawal timeline for Suboxone begins within 12 to 24 hours after the final dose and lasts between 7 to 14 days, depending on individual factors. According to Drugs.com, physical withdrawal symptoms such as nausea, vomiting, and headaches usually emerge within the first 24 hours and peak within the first 72 hours. Muscle aches, insomnia, and mood swings are common during the initial week, while depression tends to manifest more prominently during the second week of withdrawal. Drug cravings and feelings of depression persist for up to a month or longer in some individuals. Factors such as the duration of use, dosage, and metabolism influence the severity and timeline of these symptoms.
How Can I Help a Loved One with Suboxone Addiction?
You can help a loved one with Suboxone addiction by offering emotional support, encouraging professional treatment, and fostering a safe, judgment-free environment. Begin by educating yourself about Suboxone addiction and its treatment options to provide informed guidance. Encourage them to seek evidence-based therapies such as Medication-Assisted Treatment (MAT), behavioral counseling, and support groups like Narcotics Anonymous (NA) or SMART Recovery. Offering empathy without judgment reduces feelings of shame and isolation, motivating them to engage in recovery. Additionally, helping them establish routines and seek out professional healthcare services encourages a structured recovery environment. Support groups also provide shared experiences and encouragement, promoting accountability. Monitor their progress without enabling behaviors, allowing them to take responsibility for their recovery while maintaining your presence as a source of care and support.
How is Suboxone Regulated in the United States?
Suboxone is regulated in the United States by the Drug Enforcement Administration (DEA) and the Food and Drug Administration (FDA). The DEA classifies Suboxone as a Schedule III controlled substance due to its potential for abuse and dependence, although it is approved for medical use in the treatment of opioid use disorder. The FDA oversees its approval, safety, and clinical use, while the DEA enforces restrictions to ensure that Suboxone is prescribed only under proper medical supervision and as part of a comprehensive treatment plan. Additionally, the Ryan Haight Online Pharmacy Consumer Protection Act requires healthcare providers to adhere strictly to guidelines for prescribing Suboxone, preventing its illegal distribution. This regulation ensures that Suboxone is used only for therapeutic purposes and not recreational misuse, reflecting efforts to balance access to treatment with proper oversight.
What are the Dangers of Polydrug Use with Suboxone?
The dangers of polydrug use with Suboxone are severe and include increased risk of respiratory depression, overdose, and death. Polydrug use involves combining Suboxone with other substances like alcohol, benzodiazepines, or illicit opioids, which amplify the effects of each drug and lead to dangerous interactions. A press release by the FDA titled “Suboxone with benzodiazepines (e.g., Xanax) significantly raises the risk of respiratory failure” highlights that combining Suboxone with benzodiazepines (e.g., Xanax) significantly raises the risk of respiratory failure, given their depressant effects on the central nervous system. Furthermore, the combination leads to fatal overdoses, especially in individuals with underlying mental health conditions or unstable drug use patterns. According to the National Institute on Drug Abuse (NIDA), approximately 20% of Suboxone-related overdose cases involve polydrug use, emphasizing its role in treatment complications and fatalities. Safe medication management and substance counseling are important to prevent these dangers.
Is There a Link Between Suboxone Addiction and Fentanyl Addiction?
Yes, there is a link between Suboxone addiction and fentanyl addiction due to the overlapping nature of opioid dependency. Fentanyl, a potent synthetic opioid, has led to significant rates of addiction in the United States, with fentanyl addiction being highly challenging to manage. Overdose deaths of Fentanyl involving opioids rose 38.1%, as indicated by DEA.gov. Suboxone, which contains buprenorphine (a partial opioid agonist), helps treat opioid use disorder but does not eliminate the risk of cross-addiction, especially with substances like fentanyl. Individuals who have a history of fentanyl use misuse Suboxone, as the drug mimics opioid effects to manage withdrawal and cravings. According to AddictionResource.com, the presence of fentanyl increases the likelihood of treatment complications, as individuals using Suboxone for opioid replacement still experience cravings or return to fentanyl use due to its high potency.
Is There a Relationship Between Suboxone and Heroin Addiction?
Yes, there is a clear relationship between Suboxone and heroin addiction, as Suboxone is a key treatment for opioid addiction, including heroin. Heroin addiction involves intense cravings and withdrawal symptoms that Suboxone alleviates by binding to opioid receptors, reducing both cravings and withdrawal severity. Suboxone is a partial opioid agonist that acts on the same receptors as heroin, allowing individuals to transition off heroin without the same euphoric effects associated with it. According to Healthline, Suboxone has been effective in reducing heroin relapse rates by up to 50%. Many individuals use Suboxone as part of Medication-Assisted Treatment (MAT) programs to address heroin addiction, although adherence to MAT protocols is important for long-term success. Suboxone provides stabilization, but proper treatment and support are important to address psychological dependence and reduce the likelihood of relapse for heroin addiction.
How Does Suboxone Addiction Compare to Other Opioid Addictions?
Suboxone addiction compares to other opioid addictions in terms of mechanisms, treatment challenges, and prevalence. Common opioids like oxycodone, hydrocodone, and heroin lead to full opioid receptor activation, while Suboxone is a partial agonist, meaning it has a less intense effect on these receptors. Despite being used therapeutically, Suboxone still leads to dependence and addiction, with estimates showing that approximately 20% of Suboxone users develop misuse behaviors, according to Drugs.com. Comparatively, heroin addiction is associated with significantly higher rates of overdose mortality. According to the CDC, the age-adjusted rate of drug overdose deaths involving heroin decreased by 35.7% from 2.8 in 2021 to 1.8 in 2022. Suboxone provides a safer option due to its partial agonist properties, reducing risk while addressing cravings. However, other opioids like fentanyl and heroin lead to a higher rate of overdose deaths, making Suboxone a preferred choice for MAT in opioid use disorder treatment despite the challenges it presents.
How Does Suboxone Addiction Differ from Methadone Addiction?
Suboxone addiction differs from methadone addiction primarily due to its chemical properties and treatment structures. Methadone is a full opioid agonist, while Suboxone is a partial opioid agonist, leading to different levels of addiction risk and treatment profiles. Methadone addiction is associated with higher rates of physical dependence, while Suboxone has a lower risk due to its partial receptor activation. Additionally, methadone maintenance therapy is associated with longer treatment periods, while Suboxone allows for a more flexible and tapered approach. Methadone addiction has a higher prevalence rate, with estimates showing over 200,000 individuals enrolled in methadone programs compared to Suboxone’s broader use in MAT programs. These differences highlight the variety of opioid treatment options available, with Suboxone offering a less risky alternative for many patients while still maintaining therapeutic efficacy.
Hope Without Commitment
Find the best treatment options. Call our free and confidential helpline
Most private insurances accepted
Find Drug Rehabilitation Centers Near You Anywhere In the US
Addiction Resource team has compiled an extensive list of the top drug rehabilitation facilities around the country. Use our locator tool to find the best centers near you.

 FindTreatment.gov
FindTreatment.gov